Pregnancy and Postpartum in Professional Women’s Soccer
Available in:
EN
About the Author
Ella Hughes is the head of Sports Science at Portland Thorns FC, where she supports athlete profiling, performance monitoring and return-to-play decision-making in elite women’s soccer. With experience across both collegiate and professional sport, her work focuses on integrating objective testing and individualized performance strategies to support athlete health, readiness and long-term development.
Structuring Assessment and Return-to-Play with Objective Data
As postpartum return to play becomes more common and successful in elite sport, peri- and postpartum management in professional women’s soccer is now an increasingly relevant area for performance and medical teams. With more athletes returning to elite competition following pregnancy, practitioners need to support this process with the same level of structure applied to other aspects of athlete management.
…practitioners need to support [return to play postpartum] with the same level of structure applied to other aspects of athlete management.
At the Portland Thorns, this has involved developing an approach that integrates interdisciplinary collaboration, individualized athlete profiling and objective testing to guide decision-making across pregnancy and postpartum recovery.

While pregnancy is often administratively grouped alongside injury in professional sport, it is a distinct and highly individualized process. Athletes remain part of the performance system throughout pregnancy, and practitioner support should reflect that continuity.
Anchoring Decisions to Sport Demands
Effective return-to-play planning requires a clear understanding of the demands of the sport. In professional women’s soccer, match demands include repeated high-speed running, frequent accelerations and decelerations and the ability to produce and redirect force under fatigue. These demands provide the reference point for all assessment and progression decisions.

In our organization, practitioners consider multiple factors, including:
- Physical capacity
- Nutritional requirements
- Psychological adaptation
- Training history
Pregnancy alters each of these domains. As a result, the return-to-play process is built around a comprehensive understanding of the athlete rather than a single metric or test.
…the return-to-play process is built around a comprehensive understanding of the athlete rather than a single metric or test.
Role of Objective Testing in Athlete Profiling
Objective testing provides a consistent framework for tracking changes in performance capacity over time. Within this setting, testing is used to establish baseline profiles, monitor progression and inform return-to-play decisions.
ForceFrame and NordBord
ForceFrame and NordBord are used to assess isolated strength changes that commonly occur during pregnancy and persist into the postpartum period. Consistent monitoring of key regions throughout pregnancy and return to play helps inform the team about the athlete’s status and capacity for practice loads. Assessments relevant to soccer performance and postpartum recovery include:
| Systems | Tests | Metrics |
| ForceFrame | Hip Adduction and Abduction |
|
| Hip Internal and External Rotation |
| |
| Knee Extension |
| |
| Ankle Plantar Flexion | ||
| NordBord | Isometric (ISO) 30° |
|
| ISO Prone |
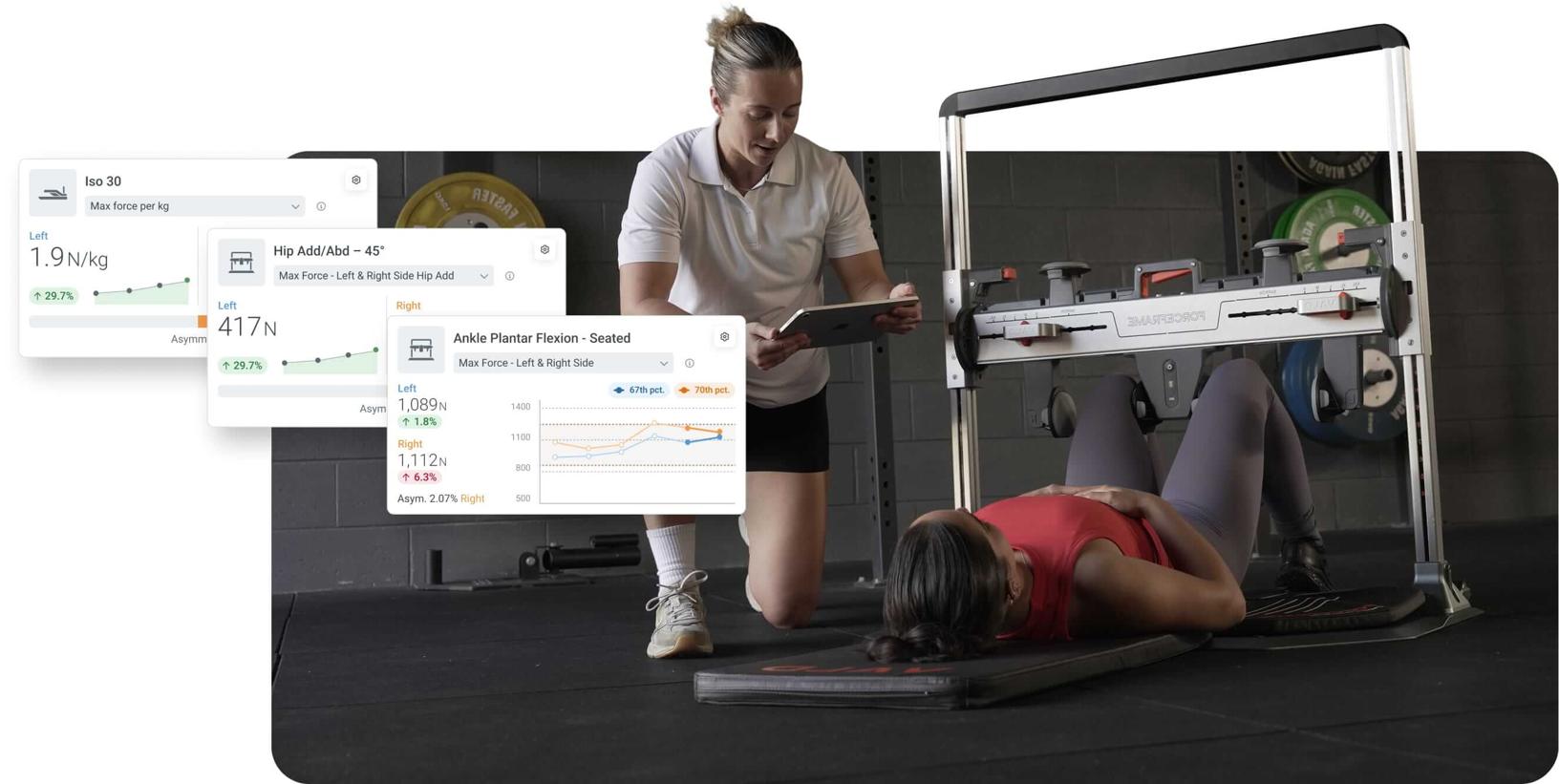
These measures provide a clear view of how specific regions are adapting throughout pregnancy and recovering after birth. This allows practitioners to identify regional deficits that may not be apparent in global movement tasks, as well as those more specific to postpartum rehabilitation, such as hip and groin strength.
[Specific assessments allow] practitioners to identify regional deficits that may not be apparent in global movement…as well as those more specific to postpartum rehabilitation…
ForceDecks
ForceDecks is used to assess isometric, dynamic and plyometric performance characteristics. In the pregnant and postpartum athlete, qualities such as jump height, deceleration capacity and jump strategy changes, including contraction times or asymmetries, help monitor athlete readiness and inform future training prescriptions. Typical assessments in our return-to-play process include:
| Systems | Tests | Metrics |
| ForceDecks | Countermovement Jump (CMJ) |
|
| Single Leg Jump |
| |
| Hop Test |
| |
| Drop Jump |
|
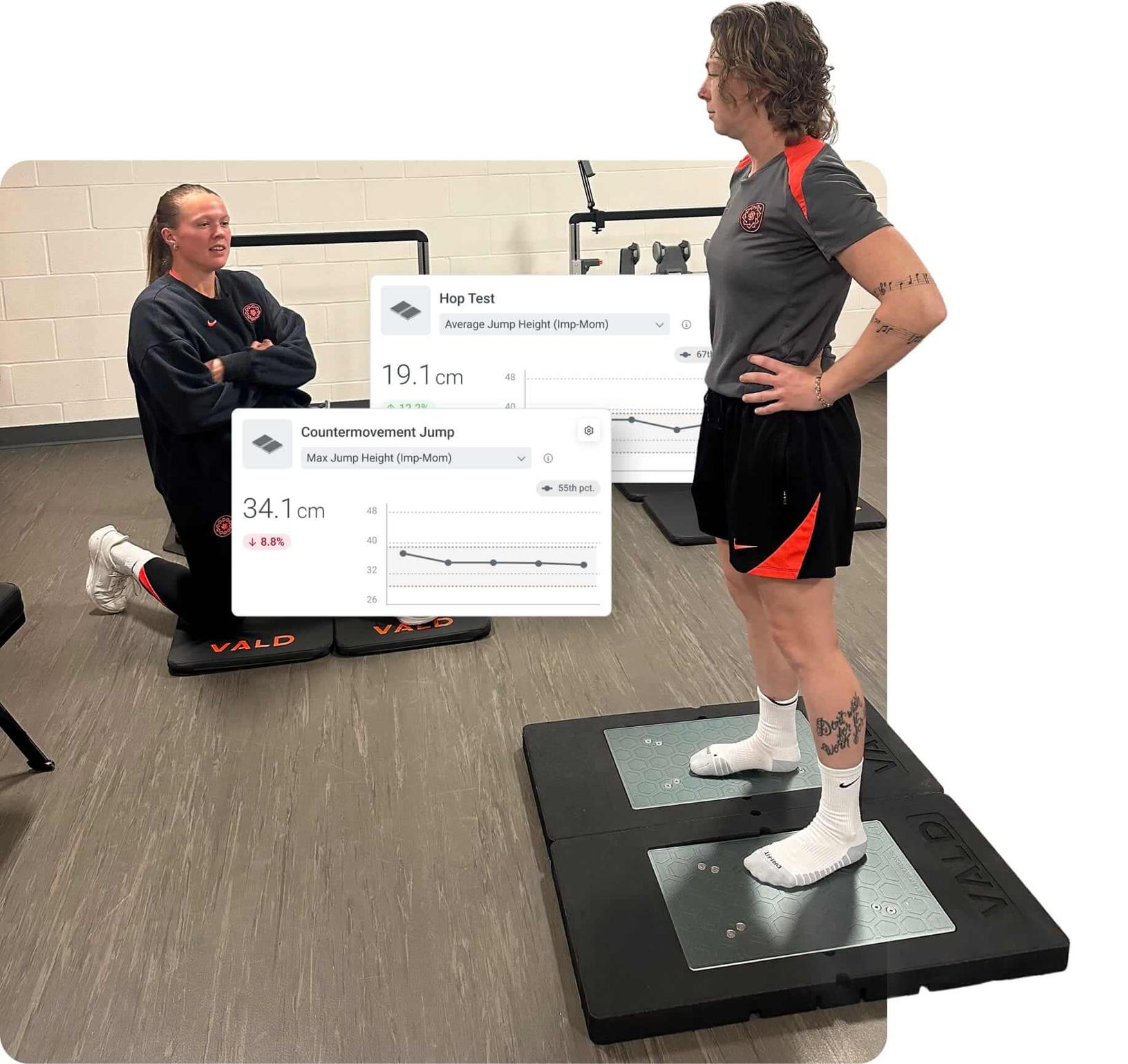
These tests are used both for ongoing monitoring and at key return-to-play checkpoints. In pregnant athletes, they help contextualize performance alongside typical time-based protocols, such as trimesters. Integrating isolated strength assessments from dynamometry with dynamic force plate testing allows practitioners to build a more complete, system-level understanding of how capacity is changing throughout pregnancy and postpartum training.
Integrating isolated strength assessments…allows practitioners to build a more complete, system-level understanding of how capacity is changing throughout pregnancy…
Postpartum Return to Play
Physical performance monitoring during and after pregnancy is guided by individual response rather than fixed trimester-based guidelines. Physiological changes, including hormonal fluctuations, shifts in mass distribution and altered movement strategies, vary significantly between athletes. As a result, assessment selection and progression are based on ongoing communication and athlete feedback.
Physical performance monitoring during and after pregnancy is guided by individual response rather than fixed trimester-based guidelines.
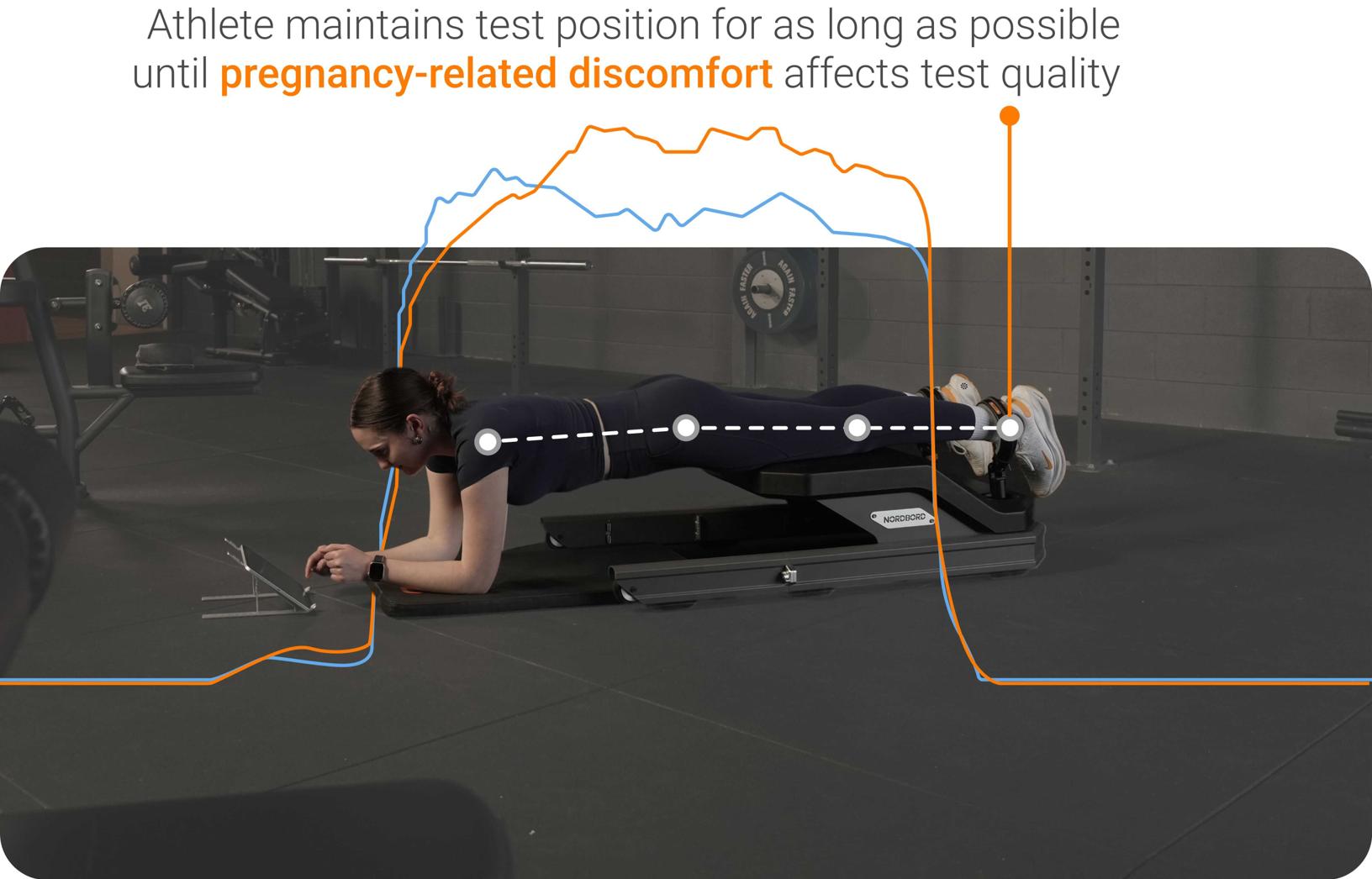
Testing procedures may be adjusted to maintain comfort and safety while still capturing relevant performance data. The goal is to preserve as much longitudinal consistency as possible without compromising the athlete. This requires practitioner flexibility and a clear understanding of the purpose behind each assessment.
Postpartum return-to-play planning begins with an understanding of the birth experience. Factors such as delivery method, duration of labor and any complications influence early recovery and progression.
From there, return to play is structured as a gradual, criteria-based process, where training exposure and performance demands are progressively reintroduced based on capacity, tolerance and objective findings. Additional considerations, including neonatal health and psychological response, further shape how and when athletes progress through each stage.
Phase 1: Early Recovery
During the initial healing phase, the focus is on building confidence and restoring basic functional capacity as the athlete adjusts to early postpartum demands. Progression is individualized and guided by factors such as delivery type and the status of internal and external healing, in consultation with the athlete’s obstetrician. This early phase typically focuses on:
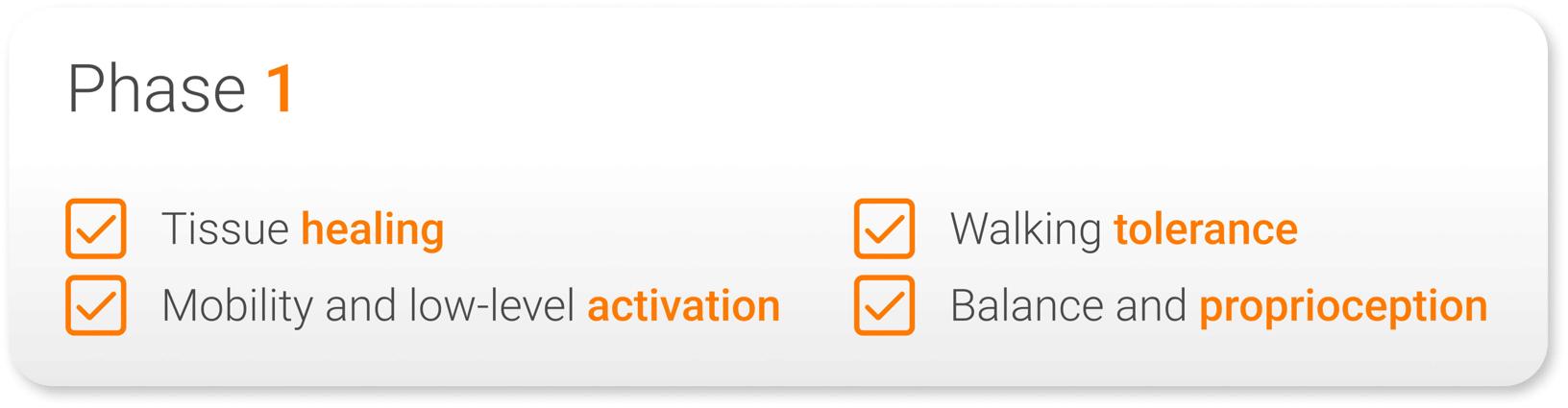
Progression is individualized and guided by factors such as delivery type and the status of [athlete] healing…
By the end of Phase 1, once bleeding has resolved, the athlete is assessed by a pelvic floor physical therapist. This assessment, alongside input from the obstetrician and broader care team, is used to determine readiness to progress to Phase 2, which often occurs around six to eight weeks postpartum.
Phase 2: Reintroduction to Training
The second return-to-play phase focuses on reintroducing foundational training while progressively rebuilding capacity and re-establishing objective testing. Key priorities during this phase include:
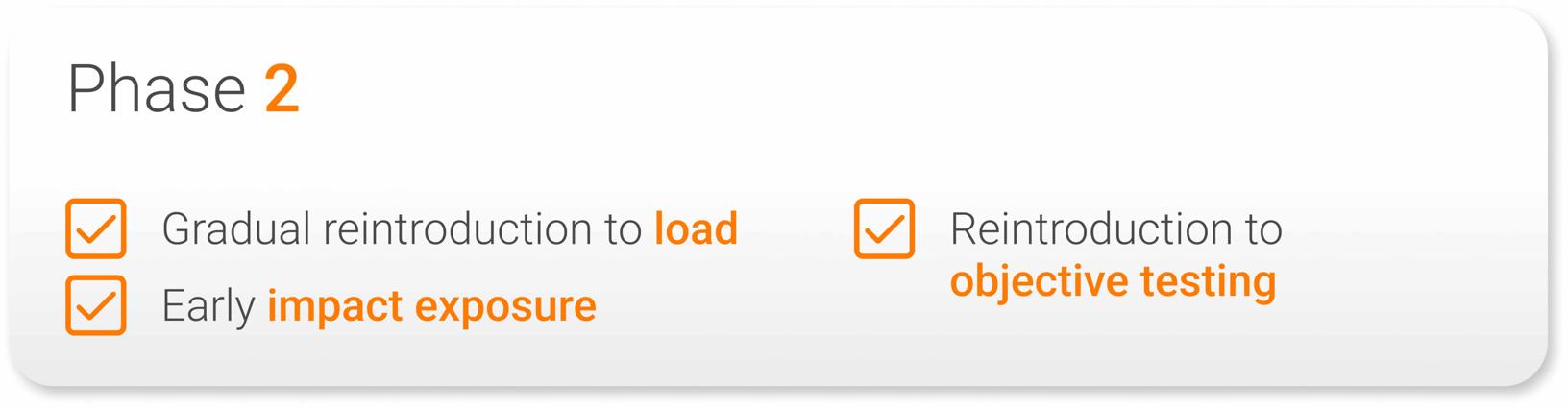
Athletes are reintroduced to familiar training patterns and positions, with testing integrated back into the weekly routine. Progression remains individualized, but the following criteria are commonly used to guide transition to the next phase:
- Strength testing values at 70-80% of pre-pregnancy levels
- Basic power capacity at 70-80% of pre-pregnancy levels
- Asymmetries < 20%
- No pain with jumping, running or lifting tasks
- Successful completion of pelvic floor assessments, guided by the pelvic floor physical therapist and individualized to the athlete’s history and demands
Phase 3: Progression to Sporting Demands
This phase progresses the athlete toward higher-intensity tasks while increasing exposure to reactive strength tasks and running demands. As intensity increases, key areas of focus include:
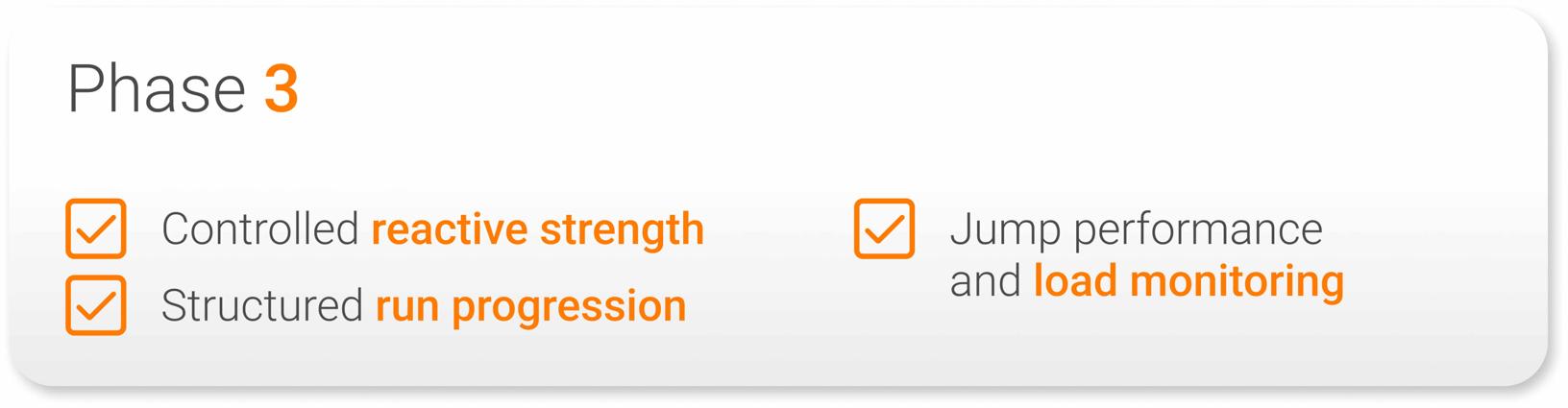
As training demands increase, ongoing monitoring of performance characteristics is used to guide load progression and assess tolerance. Progression toward return-to-sport programming is individualized, but the following criteria are commonly used to support transition:
- Strength testing values at 80-90% of pre-pregnancy levels
- Basic power capacity at 80-90% of pre-pregnancy levels
- Asymmetries < 15%
- Maximal speed at 80-85% of pre-pregnancy levels
…ongoing monitoring of performance characteristics is used to guide load progression and assess tolerance.
Phase 4: Returning to Sports Performance
This phase prepares the athlete for full return to sport by increasing exposure to sport-specific demands and reintegrating them into the team environment. Preparation for full return to sport includes:
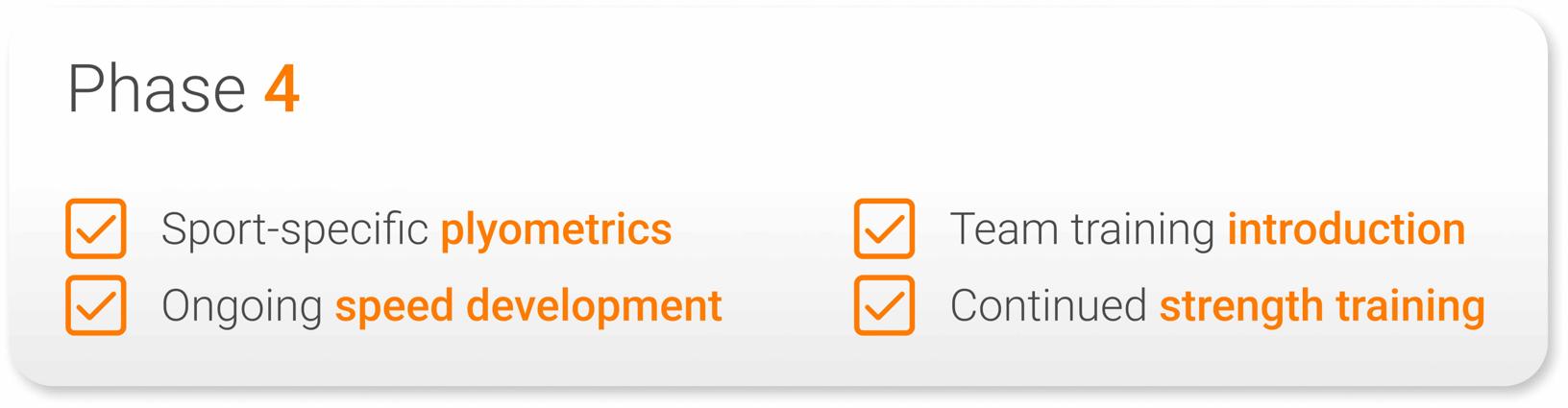
These phases provide a structured framework while allowing for individual variation based on recovery status and performance capacity. The goal is to progressively reintroduce athletes to full team demands and, ultimately, match exposure. Return-to-sport criteria are individualized, but commonly include:
- Strength testing values at 90-100%+ of pre-pregnancy levels
- Basic power capacity at 90-100%+ of pre-pregnancy levels
- Asymmetries < 10%
- Maximal speed ≥ 90% of pre-pregnancy levels
Interpreting Performance Data Postpartum and Guiding Return to Sport
Objective data helps track how performance qualities return over time. In this setting, peak power may recover relatively early, while eccentric qualities – particularly in unilateral tasks – often take longer to restore. This distinction is important, as return to sport requires both force production and the ability to control and absorb load.
Systems such as ForceFrame, NordBord and ForceDecks allow practitioners to monitor this progression through metrics such as eccentric duration, asymmetry and landing strategy. A common benchmark is returning within ~10% of pre-pregnancy strength, with tighter thresholds where appropriate.
Performance data should be interpreted within context. Factors such as sleep disruption, breastfeeding-related hormonal changes, ongoing physical demands and psychological adaptation can all influence both training tolerance and testing outcomes. These variables should be considered when planning progression, rather than relying on isolated test results.
Pregnancy and postpartum return to play requires…consistent athlete profiling, appropriate test selection and integration of both isolated and dynamic assessments.
Pregnancy and postpartum return to play requires a structured, individualized approach supported by objective data. This includes consistent athlete profiling, appropriate test selection and integration of both isolated and dynamic assessments. With reduced competition demands, this period can also be used to address long-standing limitations. Practitioners who apply a consistent, data-informed process will be better positioned to guide athletes through this transition and support return to competition.
To learn more about how objective testing can support athlete management across all stages of the performance pathway, explore the VALD ecosystem or get in touch with our team.